 Global Issues
Global Issues
Antimicrobial Resistance Calls for Brainpower of a Space Agency and Campaigning Zeal of an NGO
Nov 17 (IPS) - The cost of infectious diseases is somewhere between staggering and incalculable. Around $8 trillion and 156 million life years were lost in 2016 alone. Throughout human history, pestilences have wiped out more lives than famine and violence.
Then, in 1941, the antibiotic age was born when doctors at the Radcliffe Infirmary and the Dunn School of Pathology in Oxford first tested penicillin in a patient. When I was a medical student there in the late 1970s, we felt a reverence for this world-changing achievement. Penicillin and its successors have saved millions of lives.
So, 50 years later, as a doctor visiting Uganda’s Gulu Hospital, I was heartbroken to see patients die despite treatment with antibiotics. Sara, for example, a young Sudanese refugee, died from puerperal sepsis because she was resistant to first-line antibiotics. And modern, expensive versions were unavailable.
Antibiotics are part of a group of drugs called antimicrobials – including antivirals, anti-fungals and anti-parasitics – that prevent and treat infections in humans, animals and plants. But, as coronavirus has reminded us, all living organisms mutate. When that leads to resistant “superbugs”, we get antimicrobial resistance – the drugs are no longer effective.
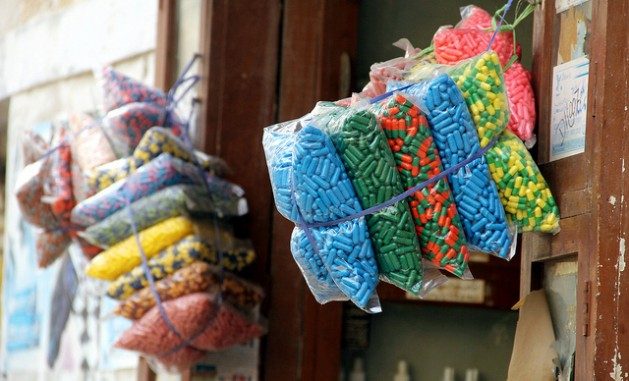
Antimicrobial resistance is a consequence of overusing and misusing antimicrobials. This is a worldwide problem. But in developing countries antibiotics are easily available without prescription. The residents of Kibera, a low income settlement in Kenya, for example, consume more antibiotics than typical American families. When a poor patient cannot afford the full course, however, they make do with a few pills. That may be harmful if an infection is not fully treated, and antimicrobial resistance may follow.
Meanwhile, the parallel lack of hygiene, water and sanitation in crowded, deprived communities means more sickness. That pushes up the need for antimicrobials.
Antimicrobial resistance also compromises human health via food. Two-thirds of all antibiotics are used in farm animals. Intensive use to fatten up animals and hide poor animal husbandry is a potent source of resistance. Powerful drugs leached into soil and water recycle into us via the food chain. Antimicrobial residues in milk, eggs, meat and fish are worrisome for our health.
Antimicrobial resistance kills around 700,000 people worldwide annually. This could increase to 10 million annually by 2050, at a cost of $100 trillion. It is a top-ten global health threat.
It’s now time for a bold effort on antimicrobial resistance. That requires a dedicated organisation with the universal legitimacy of a UN body, political clout of a G20, deep pockets of a global fund, brainpower of a space agency, campaigning zeal of an NGO, mould-breaking power of a social movement, and leveraging capacity of a public-private partnership.
Drug resistance and health
Antimicrobial resistance has devastating consequences. For the ill, it means getting sicker for longer, wasting money they cannot afford, and impoverishing desperate families. Or succumbing to ordinary chest and urinary infections that were easily treatable earlier. Traditional public health threats such as tuberculosis, malaria and HIV are also returning as serious conditions resist first-line drugs.
Drug resistance is especially bad news for seriously ill patients with diseases ranging from COVID-19 to chronic bronchitis who are prone to secondary infections. It also becomes riskier to do organ transplants or give cancer therapy because immune-suppressed patients need antimicrobial cover.
A broken market
Drug resistance satisfies the definition of a pandemic and comparison with other pandemics is instructive. Investing massively in coronavirus research was worth it because there are billions of permanent customers for COVID-19 vaccines and treatments. In contrast, nothing new has entered the antibiotics cupboard since the 1980s.
It can take 15 years and a billion dollars to develop a new antibiotic. And then, either the poor can’t afford them or consumption must be restricted to stave off future resistance. Meanwhile, companies that have monopoly rights over niche antimicrobials profit with abandon.
In contrast, 20 preventable and treatable tropical diseases that debilitate 1.7 billion poor people – mostly in Africa and South Asia – are neglected. This is because the remedies are often too cheap for sufficient profit to be extracted. They include river blindness, guinea worm, leprosy, and elephantiasis.
The particular circumstances around antimicrobial supply and demand mean that inequity prevails, as with COVID-19 vaccines where developing countries are denied the intellectual property rights to make them.
An earlier generation struggled similarly at the height of the AIDS epidemic. South Africa and India led the fight to waive restrictive trade rules on generic medicine production, when public health emergencies warrant. That saved thousands of lives as cheap antiretrovirals became available.
A comparable approach is now urgent to help all countries get effective, affordable antimicrobials. But prospects are not good, if the current battle over increasing COVID-19 vaccine supplies – led again by South Africa and India – is a pointer. Polarised geopolitics is not helpful to fix the broken market for essential medicines.
One health
The painful lesson from pandemics such as Ebola, HIV, and COVID-19 is that human, animal, and planetary health are intertwined. That is because animals are getting closer to humans. Their habitats get compromised by development practices that create wide scale deforestation. Thus, their microbes jump to us more easily. This is exacerbated by environmental shifts due to climate change. The trend necessitates new antimicrobials to be found for diseases yet to come.
Siloed approaches won’t work in inter-connected contexts. Integrated working is needed to tackle the multi-dimensional causes and consequences of our sickening humanity, ecosystem, and planet. This “one health” approach could tackle antimicrobial resistance. But the concept remains nebulous. Society and institutions don’t have incentives to work across sectoral and disciplinary boundaries.
A technocratic approach is not enough
The World Health Organisation has joined up with the World Organisation for Animal Health and the Food and Agriculture Organisation to sound the alarm on antimicrobial resistance with a global action plan, several resolutions of the World Health Assembly, and a high-level global leaders group. Technical tools and guidance are available to national action plans: 89 countries have them but only 18 in Africa and 23 in Asia-Pacific. They include strengthening surveillance, promoting antimicrobial stewardship, training and capacity building.
All this is worthwhile. But there is no time to wait. A technocratic approach and sparse funding have not created the necessary momentum.
The early AIDS activists realised the same in the 1980s when many countries were devastated, especially in Africa. A massive global movement arose to shift social morays, shake up stodgy establishments, galvanise massive funding for research, prevention, and treatment. And it triggered extraordinary innovations in biological and behavioural sciences.
Its legacy has gone well beyond HIV. It also led to the creation of UNAIDS and the Global Fund To Fight AIDS, Tuberculosis and Malaria as specialised institutions to energise and orchestrate an unprecedented global endeavour.
The hugely disruptive COVID-19 crisis has sparked comparable effort with record-time technological breakthroughs, overturned economic orthodoxy, and unprecedented financing. Also innovations in how we work, design social safety nets, re-configure international co-operation, generate solidarity, and hold policy makers accountable. But we also deepened inequalities, and realised that globalisation itself needs a makeover.
There are excellent examples of the elements that could make up a dedicated global organisation to combat antimicrobial resistance. To connect them is the necessary organisational innovation. That means challenging petty institutional turf battles and sectoral boundaries, and overcoming small mindsets.![]()
Mukesh Kapila, Professor Emeritus in Global Health & Humanitarian Affairs, University of Manchester
This article is republished from The Conversation under a Creative Commons license. Read the original article.
© Inter Press Service (2021) — All Rights Reserved. Original source: Inter Press Service